Spinal Cord StimulationSpinal cord stimulation or “SCS” offers a non-opioid, FDA-approved alternative for chronic pain treatments when other therapies such as physical therapy, medication, injections, or surgery...
Spinal Cord StimulationSpinal cord stimulation or “SCS” offers a non-opioid, FDA-approved alternative for chronic pain treatments when other therapies such as physical therapy, medication, injections, or surgery... At Home Temporary SCS SystemThe SCS trial lasts anywhere from 5 days to 14 days, depending on what your doctor decides is best for you. During the trial, consider...
At Home Temporary SCS SystemThe SCS trial lasts anywhere from 5 days to 14 days, depending on what your doctor decides is best for you. During the trial, consider... Radiofrequency AblationThis procedure uses cooled radiofrequency energy through a probe to safely target the sensory nerves responsible for sending pain signals. A radiofrequency generator transmits a small...
Radiofrequency AblationThis procedure uses cooled radiofrequency energy through a probe to safely target the sensory nerves responsible for sending pain signals. A radiofrequency generator transmits a small... Regenerative MedicinePRP stands for platelet-rich plasma, and BMAC stands for bone marrow aspirate concentration. This therapy may be used to treat various acute and chronic pain...
Regenerative MedicinePRP stands for platelet-rich plasma, and BMAC stands for bone marrow aspirate concentration. This therapy may be used to treat various acute and chronic pain...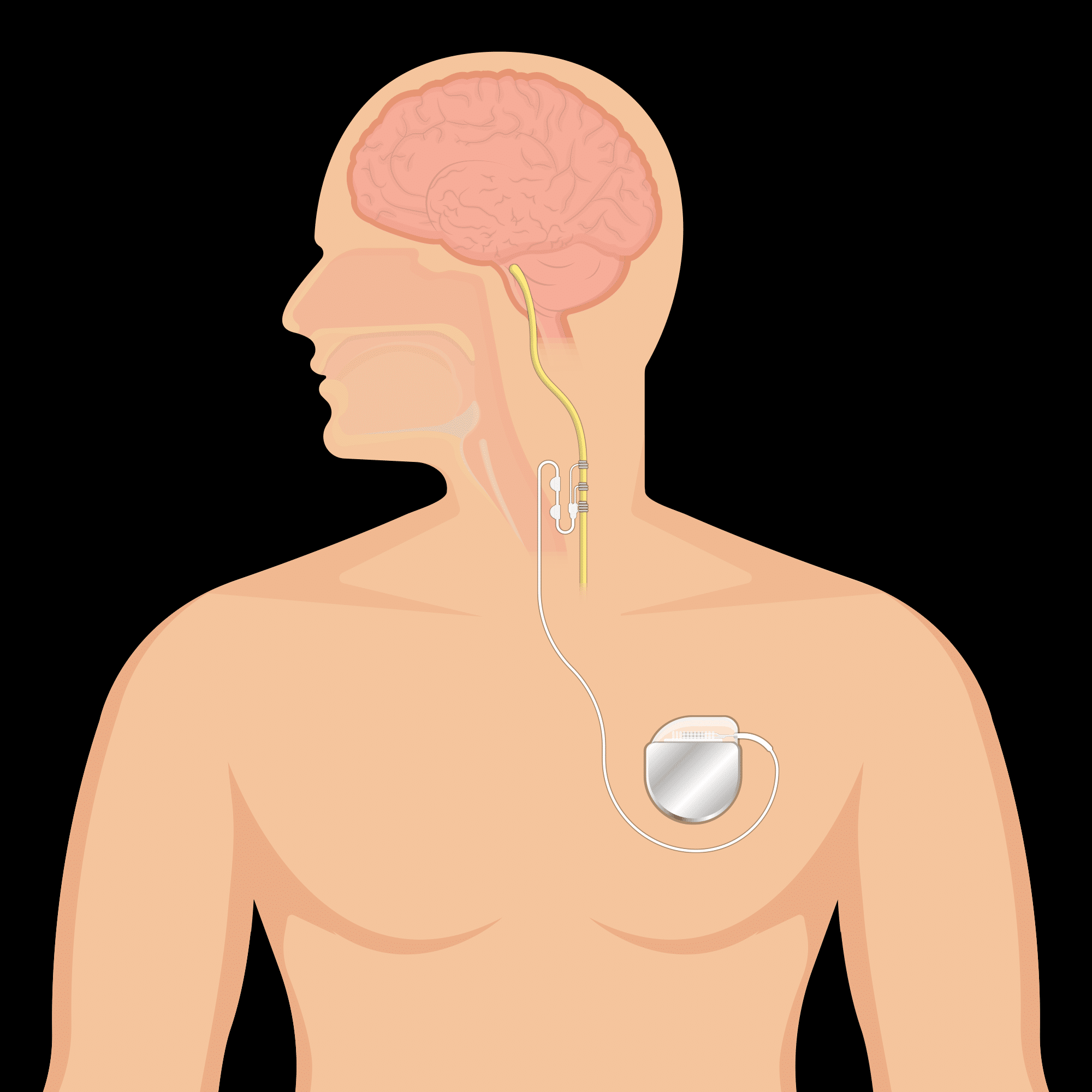 Peripheral Nerve StimulationPeripheral Nerve Stimulation provides long lasting pain relief by blocking pain signals from reaching the brain. Nerve related pain is blocked by delivering a week...
Peripheral Nerve StimulationPeripheral Nerve Stimulation provides long lasting pain relief by blocking pain signals from reaching the brain. Nerve related pain is blocked by delivering a week... Intrathecal Drug DeliveryTargeted drug delivery is a safe and effective way to manage chronic pain or cancer pain with fewer side effects and lower drug doses compared...
Intrathecal Drug DeliveryTargeted drug delivery is a safe and effective way to manage chronic pain or cancer pain with fewer side effects and lower drug doses compared... Indirect Spinal DecompressionLumbar spinal stenosis is when there is a narrowing of the spinal canal due to degenerative changes in the spine. The narrowing may cause pain,...
Indirect Spinal DecompressionLumbar spinal stenosis is when there is a narrowing of the spinal canal due to degenerative changes in the spine. The narrowing may cause pain,...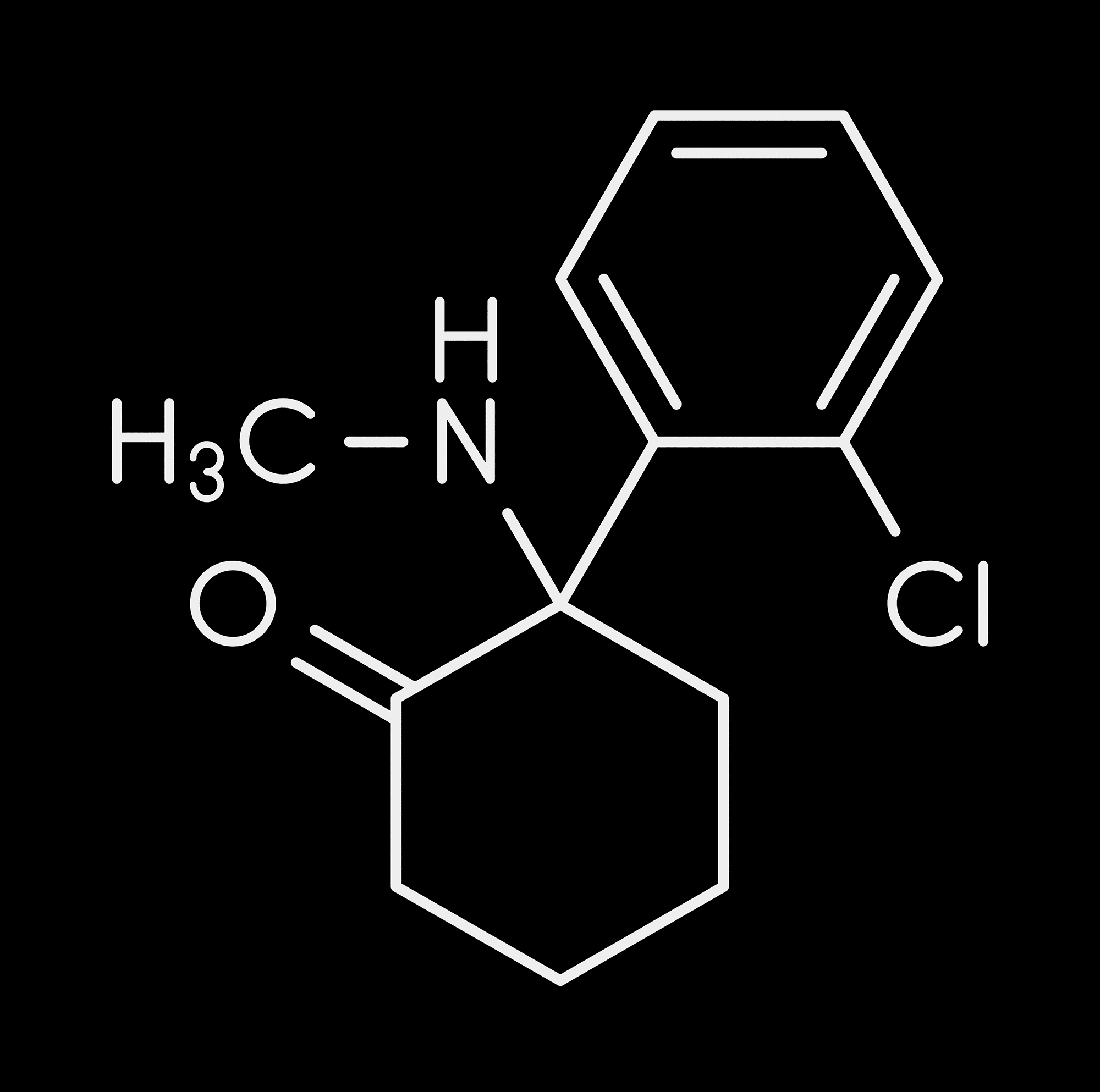 KetamineThe action of ketamine involves multiple mechanisms with multiple receptors. Ketamine is noncompetitive, reversible N-methyl-D-aspartate (NMDA) channel blocker which blocks the excited nerves, potentiates delta...
KetamineThe action of ketamine involves multiple mechanisms with multiple receptors. Ketamine is noncompetitive, reversible N-methyl-D-aspartate (NMDA) channel blocker which blocks the excited nerves, potentiates delta... Phantom Limb PainPost-amputation pain (PAP) is a challenging constellation of painful disease states caused by the surgical or traumatic removal of a limb or appendage. The most...
Phantom Limb PainPost-amputation pain (PAP) is a challenging constellation of painful disease states caused by the surgical or traumatic removal of a limb or appendage. The most...
- June 17, 2023